TREATMENT OF DEVIATED NOSE Prof. Dr. Mirza Shehab Afzal Beg
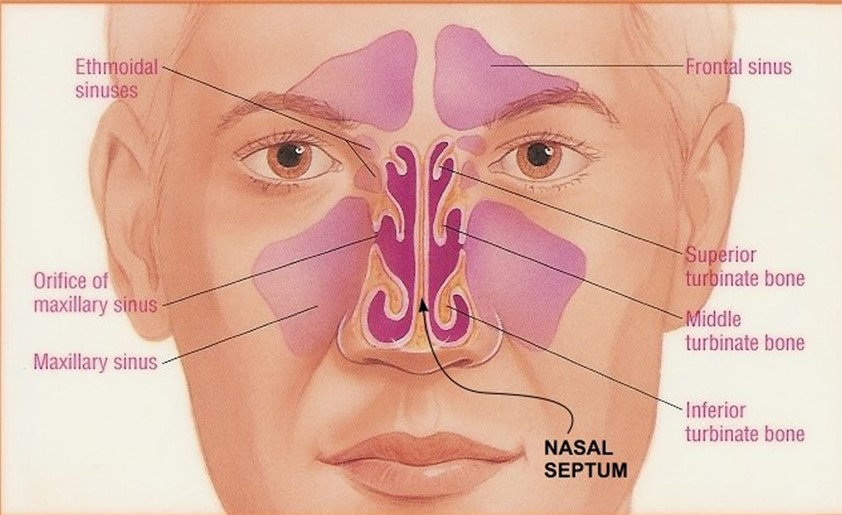
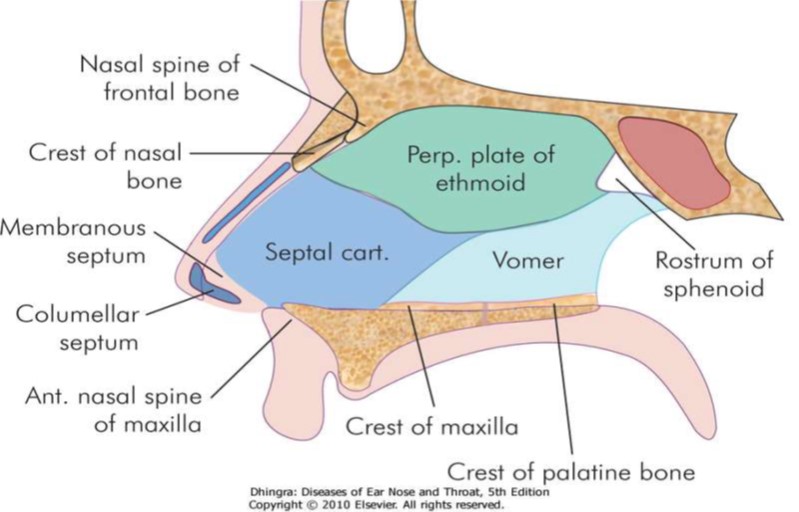
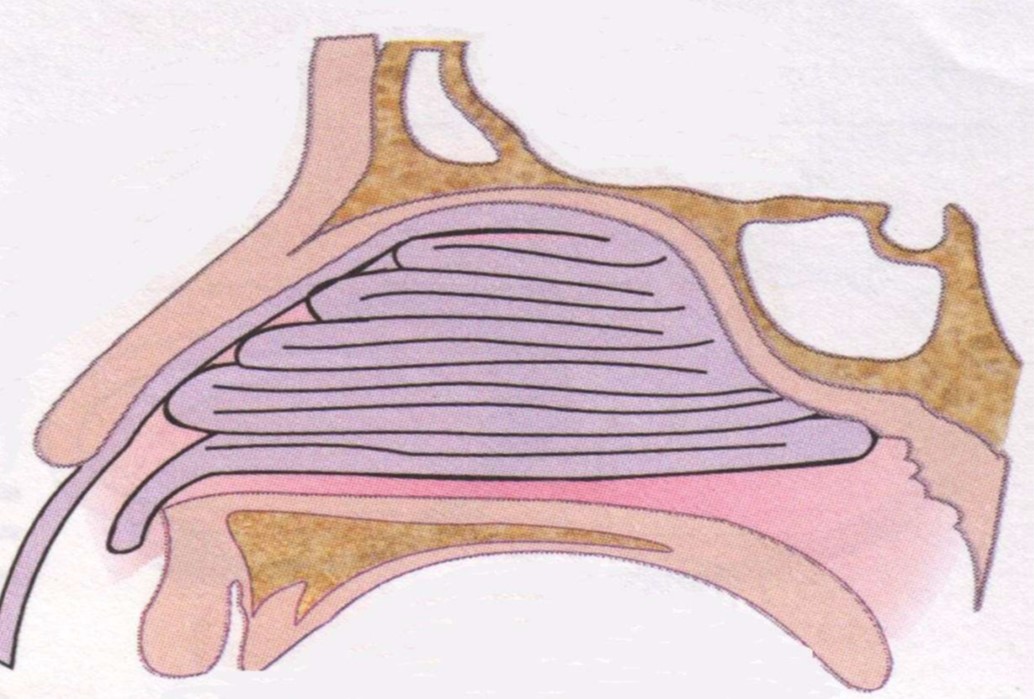
ANATOMY
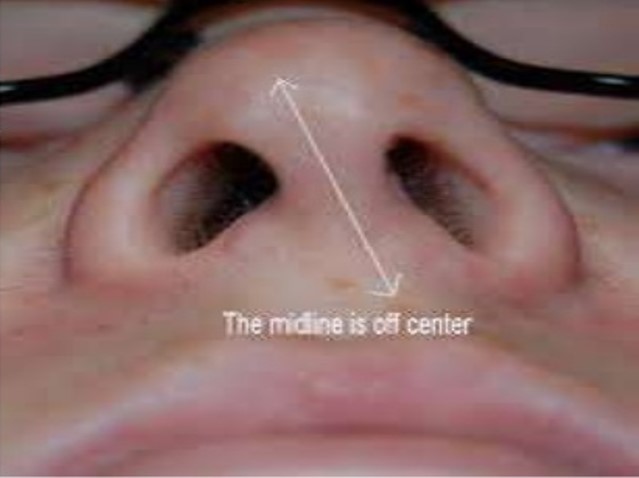
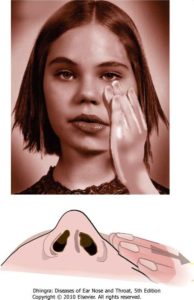
DEVIATED NOSE
- Physical disorder of the nose involving a displacement of the nose off center(external deviation)
- Causes;
- Deviated septum
- ULC-deforming forces
- Asymmetrical nasal bones
AETIOLOGY
-
- Trauma
- Developmental errors
- Racial factors
- Hereditary factors
TRAUMA
-
- A lateral blow on the nose may cause displacement of septal cartilage from the vomerine groove and maxillary crest
- A crushing blow from the front may cause buckling , twisting ,fractures and crushing of nasal septum
- Trauma during delivery
DEVELOPMENTAL ERRORS
Here’s the sentence rewritten in active voice:
“The tectoseptal process forms the nasal septum as it descends to meet the two halves of the developing palate in the midline.”
Unequal growth between palate and base of skull may cause buckling of nasal septum
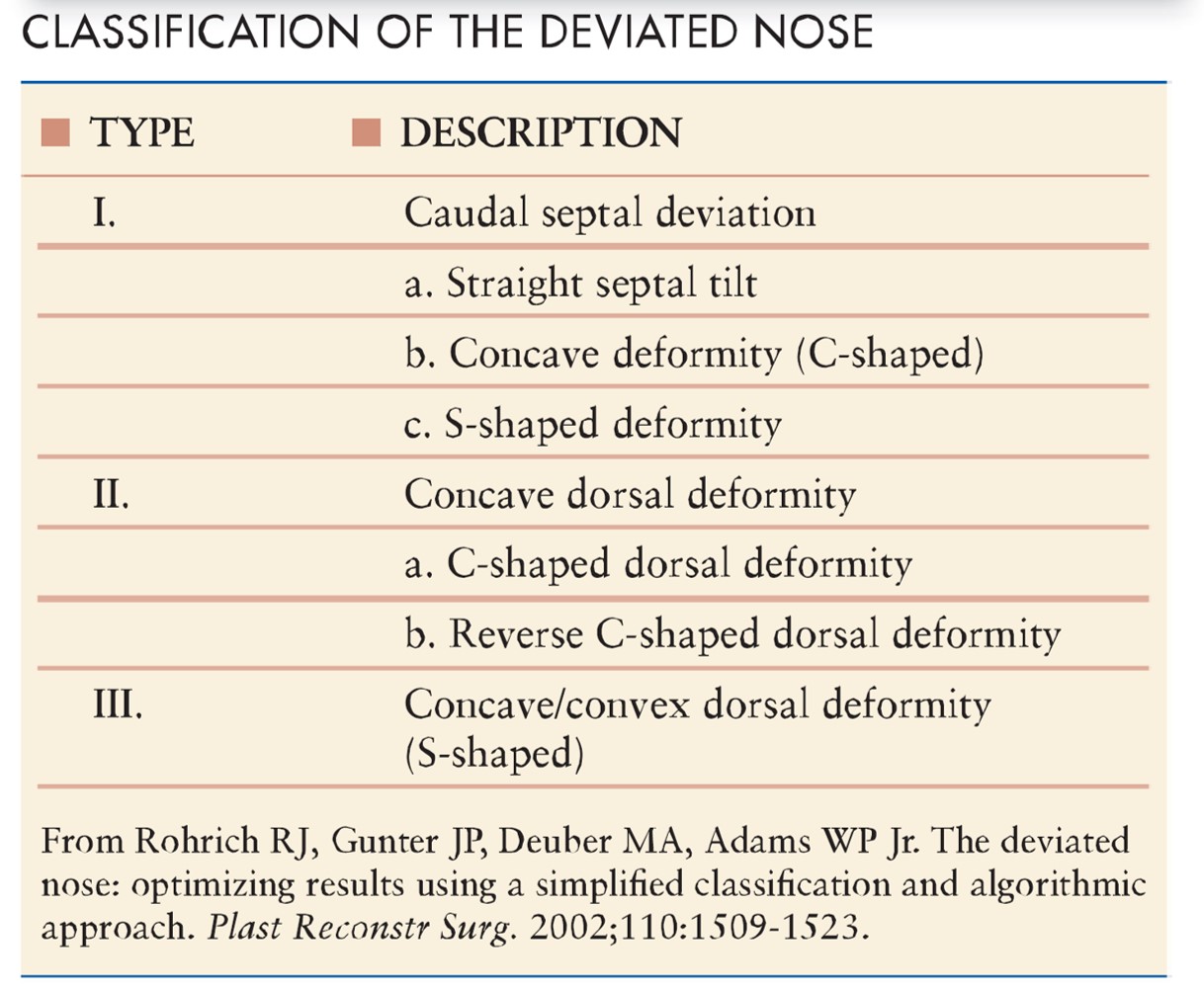
SEPTAL DEVIATION TYPES
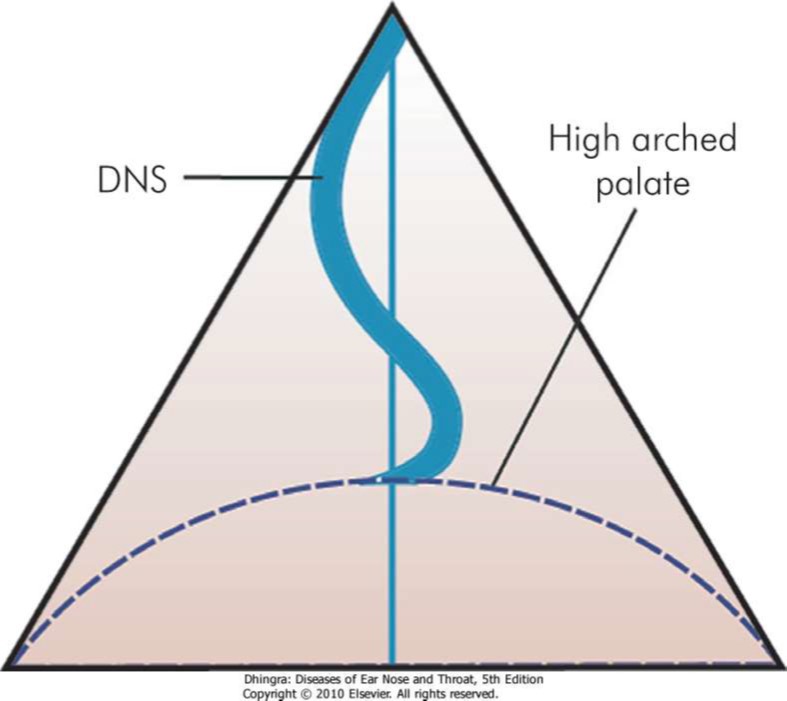
EFFECTS OF DNS
- Compensatory hypertrophy of turbinates of opposite side
- External deformity
- Impairment of drainage to sinus
- Secondary atrophic rhinitis

CLINICAL FEATURES
- Nasal obstruction
- Headache
- Sinusitis
- Epistaxis
- Anosmia
- External deformity
- Middle ear infection
COTTLE TEST
- Used in nasal obstruction due to abnormality of nasal valve
- If the nasal airway improves on test side, the test is positive
- Indicates abnormality of internal nasal valve
TREATMENT OPTIONS
- Submucous resection
- Septoplasty
- Septum repositioning
- Septal resection
- Septal scoring
- Spreader graft/Batten grafts
- Supporting sutures

SUBMUCOUS RESECTION OPERATION
Anaesthesia
local anaesthesia or general anaesthesia
Positioning
reclining position with head end of the table raised
Infiltration
subperichondrial infiltration with xylocaine with adrenaline
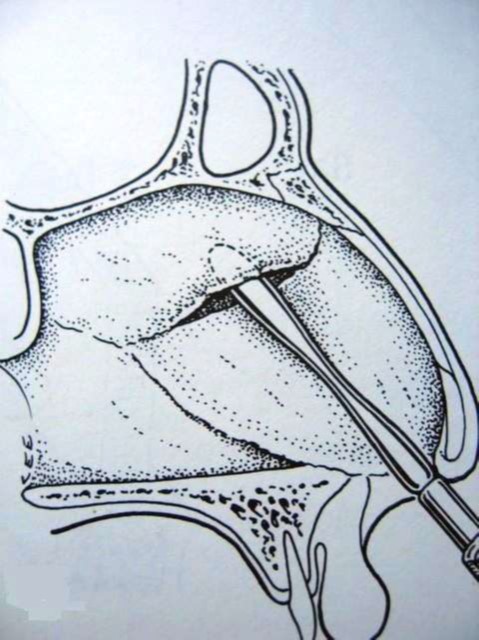
Elevation of the mucoperichondrial and mucoperiosteal flaps on either side of the septal framework
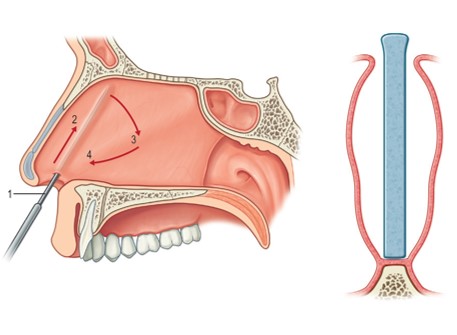
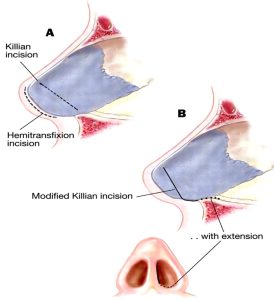
SUBMUCOUS RESECTION INCISION
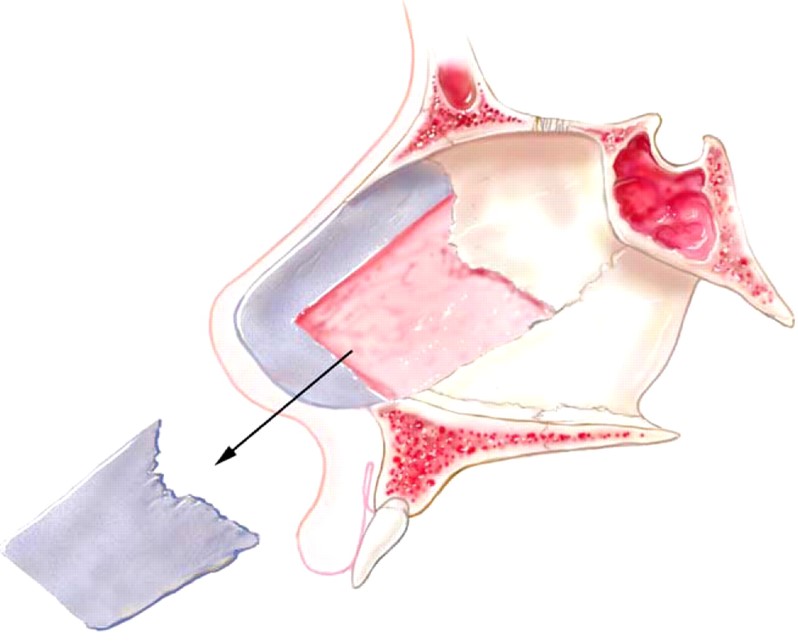
Dislocation of bony cartilaginous junction
- Removing the deflected parts of bony and cartilaginous septum, leaving a 1cm l-strut dorsally and caudally
- Repositioning the flaps
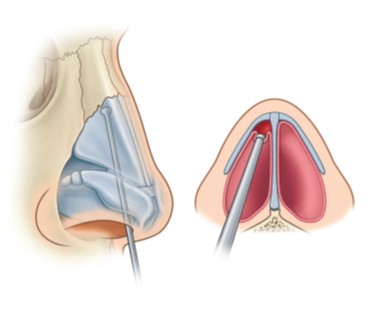
SEPTOPLASTY
- Performed under general anaesthesia in supine position
- Septal framework is corrected/resected and repositioned
- Mucoperichondrial or mucoperiosteal flap is generally raised only in one side of the septum retaining the attachment and blood supply of the other
SEPTOPLASTY INCISIONS
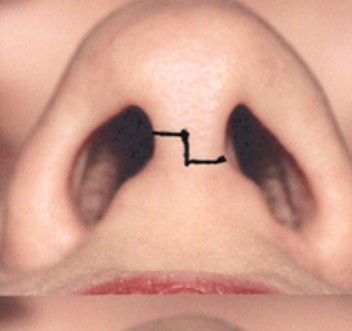
- Transcolumellar stairstep with intranasal marginal incisions: standard for open rhinoplasty
- Cartilage-splitting incision: often used in
- Intercartilaginous incision: often used in combination with marginal incision to “deliver” cartilage in closed rhinoplasty


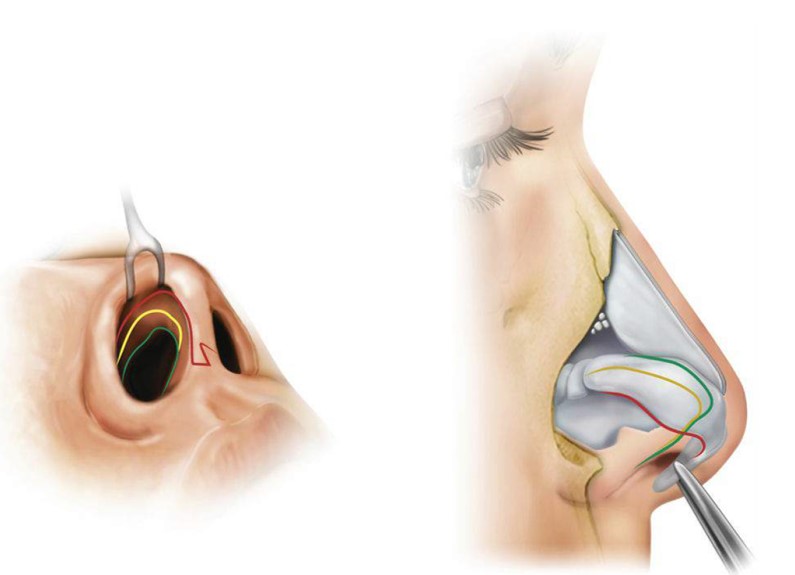
EXPOSURE
- Obtain wide exposure of the deviated structures
- Release all of the mucoperichondrial attachments of the deviated septum
- Release deforming forces, including the LLCs and ULCs from each other, and the ULCs from the septum
IDENTIFICATION OF PROBLEM
- If deviation is caused by asymmetry of the ULCs, the septal deviation can be corrected by the release of the ULCs from the LLCs
- If the deviation is result of septal deviation, the septum must be straightened
- The caudal septum must be anatomically reduced onto the nasal spine
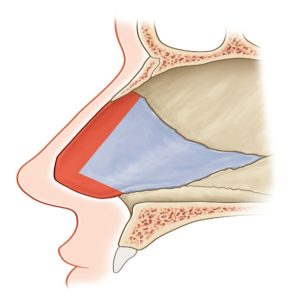
SEPTAL RESECTION
- Resection of the posterocaudal segment of the septum
- A minimum of 1 cm septal L strut (dorsal and caudal septum) must be preserved to prevent collapse of dorsum
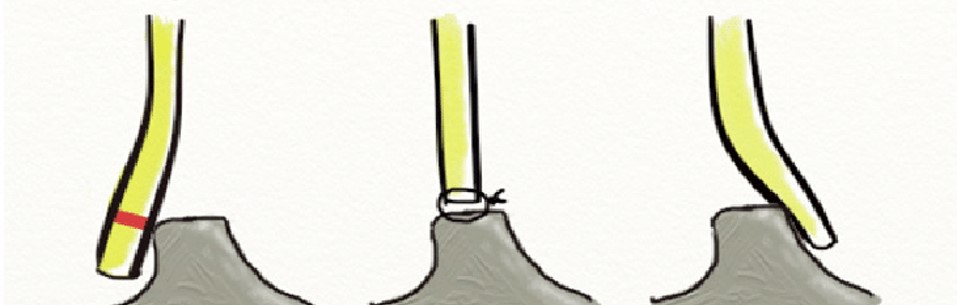
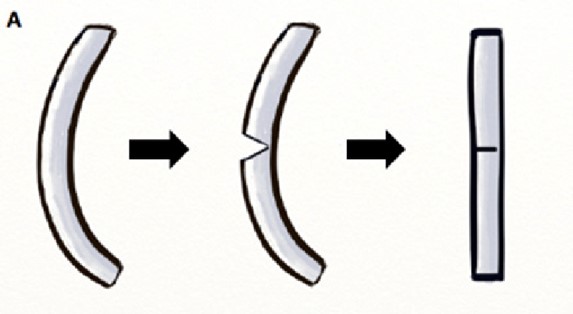
SEPTAL TILT
The surgeon removes the posteriocaudal portion of the septum, leaving an L-strut septum anteriorly and caudally
- The surgeon repositions the septum after removing a small segment of the overlapping cartilage and fixates it in the midline with a figure-of-eight suture.”
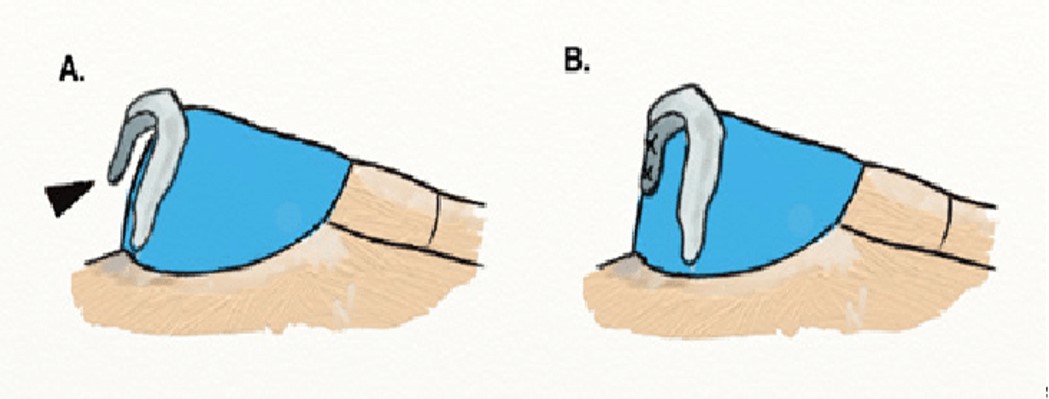
SWINGING DOOR TECHNIQUE
1.Excess septum above the maxillary crest is resected to permit repositioning in the midline
2.Caudal septum is be secured to the anterior nasal spine
which serves as a “doorstop” to straighten the septum
The caudal septum can be stabilized in the midline by its insertion into a small pocket created between the medial crura (arrowhead) in a “tongue-in-groove” fashion
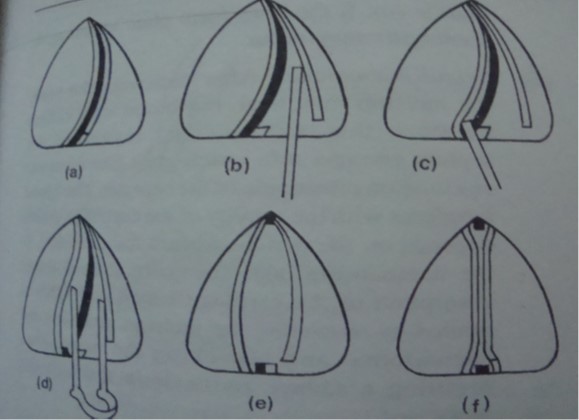
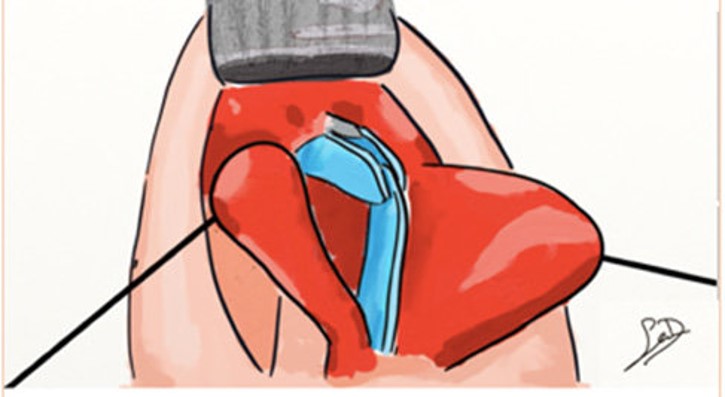
WEDGE EXCISION AND SHAVING
Small wedges of cartilage can be excised from the convex side of the deviation
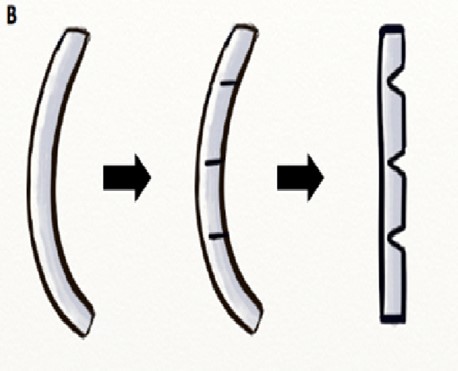
SCORING AND CROSS-HATCHING
Cartilage scoring on the concave side to destroy the cartilage memory and straighten the septum
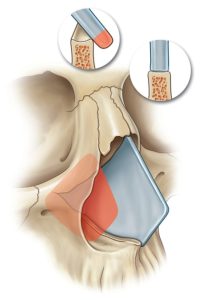
CORRECTION OF C–SHAPED SEPTAL DEVIATIONS
- Resection of the posteriocaudal portion of the septum, partial
disjunction of the perpendicular plate of the ethmoid and quadrangle cartilage and the scoring of the l-shaped frame in a cephalocaudal(a) and anteroposterior(b) direction on the concave surface - An anterior nasal spine osteotomy may also be used to correct deviation at this level
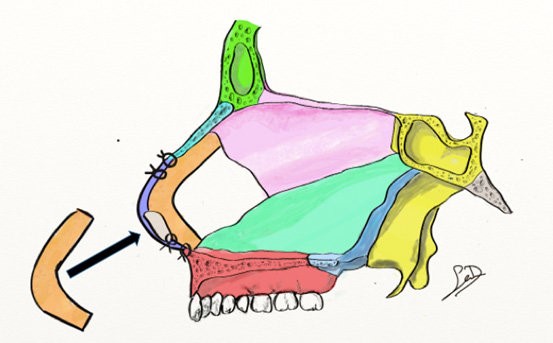
Creation of a new l-strut using bilateral extended spreader grafts that articulate with a caudal septal replacement graft.
SEPTAL BATTEN GRAFT
SPREADER GRAFT
High septal deviation: shaving the convex side of the deviation with addition of cartilage dorsal spreader grafts +/- scoring
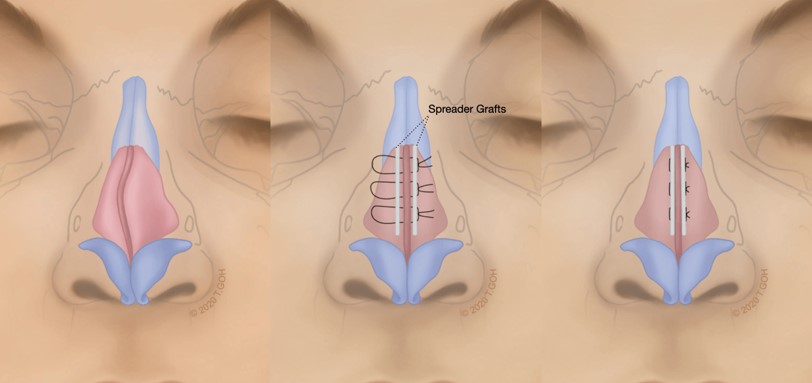
-
- “The surgeon should place bilateral cartilage spreader grafts for support and better definition of the dorsal aesthetic line if full-thickness cuts are needed.”
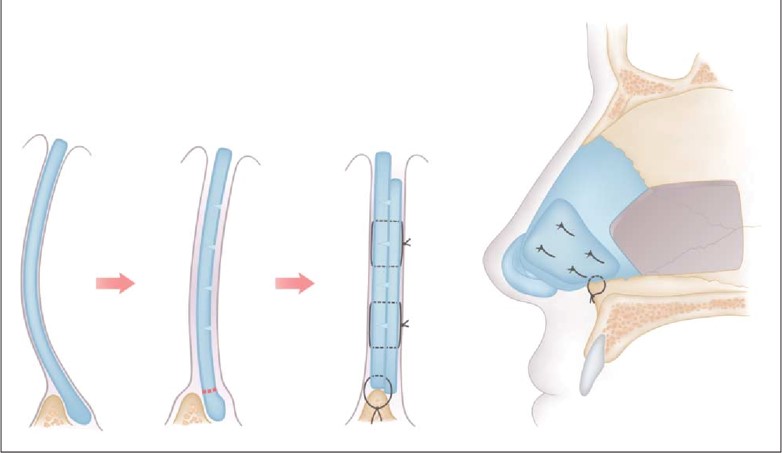
EXTRACORPOREAL SEPTOPLASTY
- Whole septum is removed, L-strut is constructed and placed back
- The neo-septum is fixated to the upper lateral cartilages and keystone region dorsally and the lateral cartilages and nasal spine caudally
ADDITIONAL PROCEDURE FOR TURBINATES
- Straightening of the septum narrows the nasal airway in patients with pre-existing inferior turbinate hypertrophy
- Options:
- Out fracture of turbinate
- Submucous resection
- Destruction via cauterization
- Steroid injection
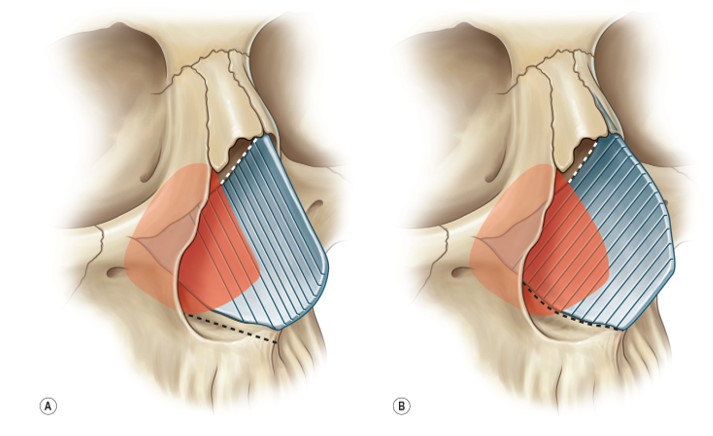
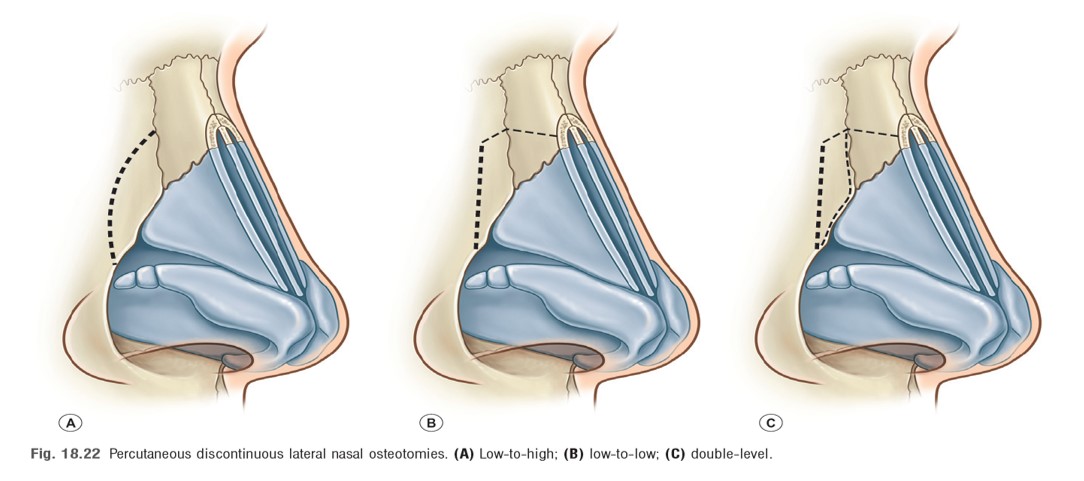
ADDRESSING THE NASAL BONE DEVIATION
- Asymmetrical oblique rasping of the nasal bones
- Osteotomies
- If the nasal bones are symmetrical, lateral osteotomies alone will be sufficient
- The surgeon may need to perform medial osteotomies if the nasal bones are asymmetrical.
OSTEOTOMIES
ANTERIOR NASAL PACKING
STERISTRIP APPLICATION

COMPLICATIONS OF SEPTAL SURGERY
- Haemorrhage
- Septal hematoma/ infection/ abscess /perforation
- Saddle nose / supratip depression/ Columellar retraction
- Collapsed septum
- Persistent deviation
- Nasal synechia
- C.S.F. rhinorrhoea
- Infection
- Toxic shock syndrome
POSTOP CARE
- Head elevation
- Nasal normal saline drops starting in the evening of procedure day
- Removal of nasal pack in 24-48 hours
- Avoidance of strenuous activities, contact sports bending head, coughing and constipation in early post op period
- Follow up in one week for ROS and steristrips, 2 weeks , 6 weeks and then in 3 months
DEVIATED NOSE TREATMENT ALGORITHM
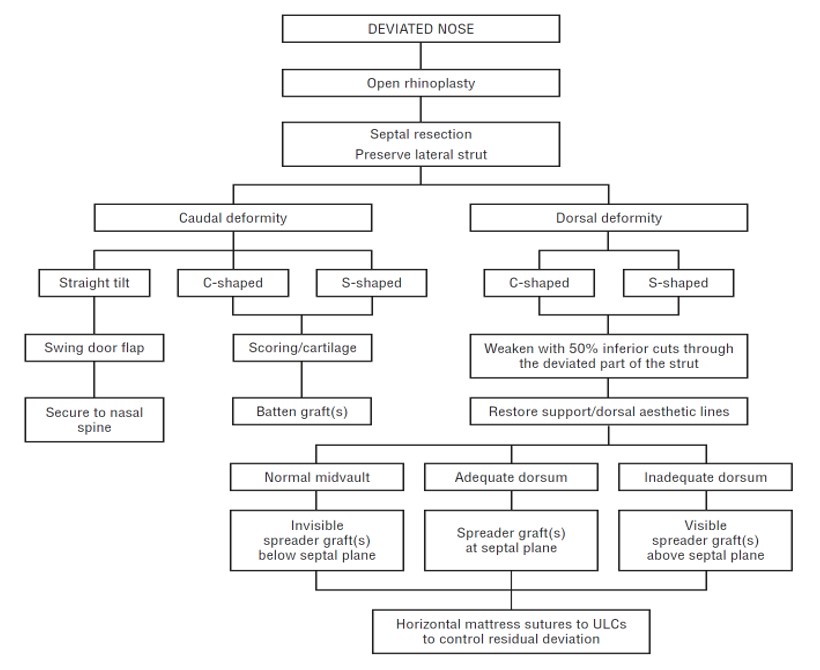
TREATMENT OF DEVIATED NOSE
Contact Us
Email ID: ahtcspk@yahoo.com
Contact no: 0323 2847513
Facebook Pages
https://www.facebook.com/Karachi-Plastic-Surgery-105404788979850
https://www.facebook.com/Dr-Shehab-Beg-Plastic-Surgeon-104382309083393/
https://www.facebook.com/Advanced-Hair-Transplant-Plastic-Surgery-102536472604336